
Scaling & polishing (Full mouth disinfection)
Full-mouth disinfection is for the treatment of gum disease. Periodontal disease affects the bone and gum that provide support for your teeth, which if left untreated can result in your teeth becoming loose and falling out.
Chronic Periodontitis is treated by removing bacteria and hard deposits that affect root surfaces underneath the gum. The aim is to complete this procedure within a short time frame of 24 hours. This is in order to minimise the chance of re-infection with bacteria coming from other areas of the oral cavity, such as tongue, tonsils and interdental spaces. This procedure is to try and minimise and stabilise the loss of bone support and tissues which help keep the teeth firm within the dentition and in the long run prevent tooth loss.
The dentist will prescribe two types of antibiotics which will need to be started a couple of days before your appointments. This helps to reduce infection and reduce the microbial load in the mouth. The Dentist will take measurements around your teeth so they can assess the severity of your Periodontal Disease. They will then explain how they intend carry out your treatment and show you techniques you can use to keep on top of Periodontal Disease.
The treatment will take two appointments. Your Dentist will treat half the mouth at each appointment as the treatment is usually done under local anaesthetic. This will make it much more comfortable for you.
During these appointments the dentist will spend a long time removing any hard tartar and soft plaque from around the teeth and under the gums. This procedure typically involves scaling and also root planing. They will also remove any extrinsic staining from your teeth. Aids of interdental cleaning will then be demonstrated to you and a customised hygiene programme will be discussed.
After your treatment and depending on the severity of your gum disease—you will be asked to return in 2 months so we can again measure around your teeth and assess how healthy your gums are, whilst also assessing your progress on home cleaning. At this appointment, your teeth will be cleaned again removing any reformed plaque
Sufficient treatment for periodontal disease has never been so important. There are a number of links proven between periodontal disease and other health problems. Just to name a few… Heart Disease pre-term low birth weight children Diabetes Rheumatoid Arthritis Obesity Alzheimer’s Disease.
The success of your periodontal treatment relies highly on excellent oral hygiene. This is why it is so important that you take into account all of the information advice and aids recommended to you by your Dentist.

Local drug delivery
In order to complement non-surgical therapy in periodontitis, there are multiple options of antimicrobials, such as metronidazole, chlorhexidine, minocycline, doxycycline and tetracycline, which can be locally delivered into the mucosa. These drugs are used in periodontal pockets and can inhibit or eliminate periodontopathogenic microorganisms as well as modulate the inflammatory response of tissues. However, limited data are available concerning the relationship between effect, efficacy and clinical status of the periodontium, chlorhexidinegluconate, doxycycline hyclate, metronidazole gel, minocycline ointment and tetracycline fibers, were reviewed aiming to address the mechanism of action and the evidence of clinical effectiveness of adjunctive use of these antimicrobials following surgical and/or non-surgical therapies. The adjunctive use of local drug delivery systems with controlled release properties may provide a defined, but limited, beneficial response on periodontal pockets. Furthermore, local drug delivery as an active treatment or maintenance therapy depends on clinical findings, responses to treatment described in the literature, desired clinical outcomes, and patients' dental and medical histories, including their past usage of antimicrobials.

Gum (Flap) surgery
You may need surgery for severe gum disease (periodontitis) if it cannot be cured with antibiotics or root planing and scaling. A flap procedure cleans the roots of a tooth and repairs bone damage caused by gum disease. A gum specialist (periodontist) or an oral surgeon often performs the procedure.
Before the procedure, you will be given a local anesthetic to numb the area where the doctor will work on your gums.
The doctor will pull back a section of your gums to clean the roots of your teeth and repair damaged bone, if needed. The gum flap will be sewn back into place and covered with gauze to stop the bleeding.
Bone may be:
Smoothed and reshaped so that plaque has fewer places to grow.
Repaired (grafted) with bone from another part of the body or with man-made materials. The doctor may place a lining on the bone graft to help the bone grow back. The lining may need to be removed later.
What to Expect after Surgery ??
Repaired (grafted) with bone from another part of the body or with man-made materials. The doctor may place a lining on the bone graft to help the bone grow back. The lining may need to be removed later.
Take painkillers as prescribed.
After 24 hours, you can rinse your mouth gently with warm salt water several times a
day to reduce swelling and relieve pain. Change gauze pads before they become soaked
with blood. Relax after surgery. Strenuous physical activity may increase bleeding.
Eat soft foods such as gelatin, pudding, or light soup. Gradually add solid foods to
your diet as the area heals. Do not lie flat. This may prolong bleeding. Prop up
your head with pillows. Continue to carefully brush your teeth and tongue. Apply an
ice or cold pack to the outside of your mouth to help relieve pain and swelling. Do
not use sucking motions, such as when using a straw to drink. Do not smoke. A few
days after the procedure, your dentist will remove the stitches.
Repaired (grafted) with bone from another part of the body or with man-made materials. The doctor may place a lining on the bone graft to help the bone grow back. The lining may need to be removed later.
Why is it done ??
The flap procedure is necessary when severe gum disease (periodontitis) has damaged the bones that support your teeth.

Laser Dentistry
LASER dentistry using light beam with precision to remove decay. Shot less, without drill for all procedures. Our clinic is one of its own kind of dental clinic in Ahmedabad.
Lasers are used to correct vision, treat skin conditions, and perform surgery. The use of Lasers is already a trend in dentistry since last couple of decades; it was not until recent that a dental “Hard tissue” laser was perfected to be able to cure tooth decay. NO NEEDLE, NO DRILL, NO DISCOMFORT! Mostly, noise less and safest treatment which make a mild popping sound, “Like a popcorn popper”, as they vaporize decay.
The laser puts the tooth to sleep just by focusing light and water on the tooth. It then vaporizes the decay and sterilizes the remaining tooth structure. A filling is then placed and the tooth is fixed. Multiple procedures can also be done in one appointment.
All ages of children and teens like the idea of no needle and no pain to have a cavity filled. Our lasers do this every day
Treatment with the laser does not cost you more! Whether it’s tooth decay, canker sores, tongue ties, overgrown gums, or attachments that cause teeth not to properly grow together namely “frenum”, our lasers can comfortably handle the problem.
Laser soft tissue surgery using a precise light beam to correct “tongue tie” or “lip tie.these procedures can assist in improving infant nursing, proper speech, eating and swallowing issues and other concerns.
Our clinic is proud to offer this wonderful dental technology as an option to our patients seeking gum recon touring treatment. Laser dentistry has been a fantastic tool in modern dentistry and continues to improve the lives of countless people.
Laser dentistry can also be used for more than just "aesthetic" artistic dentistry. It can be used to help diagnose cavities and even treat gum disease!
The dental laser is a very versatile tool that can often take the place of a dental drill to provide patients with more comfort, faster recovery, and added precision and efficiency.
We are excited to be able to offer laser dentistry to help you and your loved ones achieve your dental goals.

Frenectomy
A frenectomy is a surgical procedure performed to remove a section of the frenulum, usually as a dental procedure. The frenulum is a type of tissue that connects the lips and tongue to the jawbone. It may be too short, long or tight and need surgical intervention.
There are 2 different types of frenulum in the mouth, the lingual frenulum located beneath the tongue and the labial frenulum which is located along the upper and lower gums and lips.
Problems with the lingual frenulum are common among children as the frenulum may be too tight which can caused problems with speech, and is often referred to as being tongue-tied.
A labial frenectomy is commonly performed on patients who require dentures or Envisaging, as the frenulum may cause irritate the dentures or may be attached high up on the gums. It can help with gum recession or with removing space between the teeth.
Recommended for:
- Babies born with a short, long, or tight frenulum which may cause difficulty breastfeeding
- Patients who have speech difficulties as a result of the frenulum
- Patients who are being fitted with dentures or braces may require a labial frenectomy

Splinting of mobile teeth
The ligating, tying, or joining of periodontal involved teeth to one another in order to stabilize and immobilize the affected teeth.
Mobile lower anterior teeth is a common complaint of dental patients with fairly advanced periodontal disease. The treating of these mobile teeth is often not very successful. The mobility is caused by a loss of supporting bone around the roots of the teeth. Even comprehensive periodontal treatment cannot replace this missing bone and the prognosis for these teeth is poor. In the majority of cases the lower four incisors (the four teeth between the two lower canine teeth) are the teeth showing the first signs of mobility.
The most logical way to treat the mobility once the active periodontal disease is under control would be to splint these mobile teeth. Various methods of splinting are employed by dentists. The most frequently used technique is to use orthodontic stainless steel wire, bonded on to the lingual surface (or inside) of the teeth with composite (white filling material) which acts as a splint. This method has some success but the metal wire is quite rigid, and this type of splint tends to de-bond and fail in time. Another disadvantage of this technique is that there is no true bonding between the metal wire and the composite filling material. There can also be aesthetic compromises with this technique, but the concept is good and these splints are an option if nothing better is available.
The other options are mostly quite invasive and non-reversible. They can involve:
- The extraction of the mobile teeth, and replacing the extracted teeth with a removable, partial denture.
- Cast precious metal splints.
- Extractions of the mobile teeth and replacement with dental implants. This may not be possible as these may require expensive and technique sensitive bone grafting procedures to provide a bony foundation for the implants as bone is lost in the periodontal disease.

Crown lengthening ( With / Without bone removal )
This is a surgical dental procedure involving the removal of gum tissue and bone to expose more tooth surface area.
Why is Crown Lengthening performed?
Crown lengthening is often performed when a tooth needs to be fixed, but not enough of the tooth protrudes above the gum to support a filling (restoration) or crown. This can happen when:
A tooth cracks off at the gum line. A crown or filling falls out of a tooth and there is tooth decay underneath. A tooth has decay below the gum line.
Crown lengthening can also be used in cosmetic dentistry to fix a "gummy smile" – when a patient has a lot of gum tissue around their upper teeth. Excess gum tissue is removed to create a more aesthetically pleasing appearance. For more information, click on the gummy smile link.
Before the surgery, the patient may require a professional tooth cleaning. If the patient needs a crown, the surgeon may place a temporary crown. The temporary crown protects the tooth and allows the surgeon to gage how much soft tissue or bone to remove.
How is Crown Lengthening performed?
The crown lengthening procedure is performed under local anesthesia. The periodontist will cut and peel the gums away from the teeth to expose the roots of the teeth and the surrounding bone. The surgeon will then remove gum tissue and sometimes bone from around the roots of the teeth. Bone is removed using a combination of hand instruments and rotary instruments. Once enough of the tooth has been exposed, the area will be irrigated with sterile salt water and the gums will be stitched together. The periodontist may cover the surgical site with a dressing called an intraoral.
Even if only one tooth needs crown lengthening, the surgeon may include neighbouring teeth so that the gum tissues are evenly reshaped. Post-surgery, the teeth will appear elongated because the gums are now shorter than before the surgery.
You will be given prescriptions for a pain reliever and a mouth rinse. Your dentist will ask you to follow a somewhat soft diet. You can brush the teeth near the stitches, but avoid the gums. Remove food particles with a toothpick or a water irrigator.
The periodontist will prescribe pain medication and a chlorhexidine mouth rinse. An ice pack may be placed against the face to reduce swelling. The patient will be instructed in post-surgery care, and scheduled to return in 7 to 10 days for follow-up. The gums will be allowed to fully heal for one month then the tooth is prepared for the restoration or final crown.

Osteoplasty & Ostectomy
Accessing the tooth roots in periapical surgery (PS) requires the elimination of periapical bone.
To compare the postoperative morbidity and prognosis following PS on mandibular molars by ostectomy, or by osteotomy with repositioning of the vestibular cortical.
CONCLUSIONS:
There was no statistically significant relationship between the surgical procedure used and post-operative pain or prognosis. Patients who underwent an ostectomy presented more swelling than those who were treated with an osteotomy and repositioning of the vestibular cortical.
Successful treatment of periodontal disease can be achieved today through a number of surgical and nonsurgical procedures, each aiming to control infection and inflammation and reduce pocket depth. Periodontal surgery can still be considered a keystone in the treatment of periodontitis. Osseous resective surgery is defined as a means of changing the diseased tissue contour to reproduce a more physiologic anatomy. Knowledge of the pathogenetic mechanisms of the disease process and identification of the defect characteristics enable the clinician to select the appropriate surgical therapy to correct the deformity and establish a healthy environment.
The degree of destruction of periodontal tissues involving bone, periodontal ligament, cementum, and connective tissue depends on several factors such as type of bacteria, host response, teeth anatomy, hard and soft tissue biotypes, and so forth. Once the lesion has progressed apically, a discrepancy between the gingival margin and bone contour is established, resulting in a pocket. The characteristics of this pocket are determined by gingival biotype, morphology of the osseous crest, and teeth anatomy and location. As the inflammation caused by the periodonto-pathogens moves apically in the periodontal apparatus, a change in the anatomy of the zone takes place. If the bone is thick enough, a funnel-shaped defect is created while the surrounding bone not involved in the demineralization process maintains the gingival tissue in the same position. In the case of thin bone, such as buccal bone or interproximal bone between mandibular incisors, a horizontal pattern of resorption usually takes place, and depending on the soft tissue thickness, a recession or a suprabony pocket is formed.

Vestibuloplasty
In general, a vestibule is an entry way between the outside and inner chambers, and in the mouth, refers to the space between the inside of the lips and the teeth. A Vestibuloplasty is a dental surgery usually considered only when there is insufficient bone and/or tissue to support dental prosthesis like dentures and implants.
Vestibuloplasty is a comprehensive range of surgical procedures, usually done by an oral or maxillofacial surgeon, to increase the height and width of the alveolar ridge of bone and gum tissue that holds the teeth, to provide sufficient structure to securely hold dentures or dental implants.
When all teeth are missing and dentures are being worn, the gums and underlying bone typically decease, because lacking tooth roots to stimulate the bone and keep it healthy and whole, the body reabsorbs the bone and it immediately begins to shrink both horizontally and vertically. The membranes and tissues covering the bone also become diminished. This, in turn, causes dentures to become loose and need refitting for new dentures. Dentures can be relined, but unfortunately that is only a temporary fix to postpone the surgery.
Partial extraction therapy (PET)
Partial Extraction Therapy (“Pet™”) Is An Advanced Procedure Used For The Creation Of A Socket Shield And Should Only Be Performed By Licensed Dental Professionals With The Requisite Skill, Education, And Due Care And Who Have Received Formal Training On Both This Procedure And The Placement Of Dental Implants.
Dentists and patients are regularly confronted by a difficult treatment question: should a tooth be saved through root canal treatment and restoration (RCT), be extracted without any tooth replacement, be replaced with a fixed partial denture (FPD) or an implant-supported single crown (ISC) ?
The purpose of this systematic review was to compare the outcomes, benefits, and harms of endodontic care and restoration compared to extraction and placement of ISCs, FPDs, or extraction without tooth replacement.
Evidence tables were developed following quality and inclusion criteria assessment. Pooled and weighted mean success and survival rates, with associated confidence intervals, were calculated for single implant crowns, fixed partial dentures, and initial nonsurgical root canal treatments

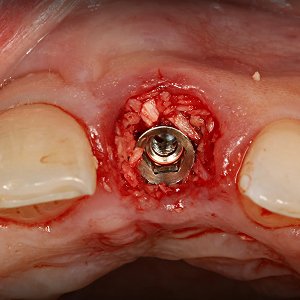
Socket preservation (Prevent bone loss after extraction)
Preserving Your Jaw Bone after Extraction
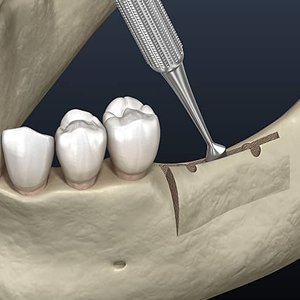
Removal of teeth is sometimes necessary because of pain, infection, bone loss or fracture of the tooth. The bone that holds the tooth in place (the socket) is often damaged by disease and/or infection resulting in deformity of the jaw after the tooth is extracted. In addition, when teeth are extracted, the surrounding bone and gums can shrink and recede very quickly after the extraction resulting in unsightly defects and collapse of the lips, and cheeks.
These jaw defects can create major problems in performing restorative dentistry whether your treatment involves dental implants, bridges or dentures. Jaw deformities from tooth removal can be prevented and repaired by a procedure called socket preservation. Socket preservation can greatly improve your smile’s appearance and increase your chances for successful dental implants for years to come.
Several techniques can be used to preserve the bone and minimize bone loss after an extraction. In one common method, the tooth is removed and the socket is filled with bone or bone substitute. It is then covered with gum, artificial membrane, or tissue stimulating proteins to encourage your body’s natural ability to repair the socket. With this method, the socket heals eliminating shrinkage and collapse of surrounding gum and facial tissues. The newly formed bone in the socket also provides a foundation for an implant to replace the tooth. If your dentist has recommended tooth removal, be sure to ask if socket preservation is necessary. This is particularly important if you are planning on replacing the front teeth.

Guided bone regeneration (GBR) to increase the volume of bone
Implant dentistry is becoming an increasingly popular treatment choice. In order to achieve a long -term, predictable prognosis, eligible implant patients must have adequate bone volume. Many patients lack sufficient horizontal or vertical bone, but there are various methods that can be used to augment new tissue growth and increase bone volume in these cases. Guided Bone Regeneration (GBR) is a technique that provides space for new bone using barrier membranes. These spaces can then be filled with new, guided bone growth. When used to fill in bone defects with new bone, GBR can provide the best, most predictable results and this technique helps to provide long-term stability to the augmented site.
The concept of GBR was originally introduced many decades ago. Experiments at that time focused on regenerating nerves and tendons. Later, a series of studies showed GBR could predictably provide new bone regeneration and healing of bony deficits around dental implants, thereby increasing the width and height of alveolar bone.
Effectively chosen membranes will be porous to allow essential nutrients, fluids, bioactive materials and oxygen to pass through, but will also be impermeable to epithelial cells. Pore size is vitally important. A pore size that is too large will permit epithelial cells to overpopulate the space, inhibiting the growth of bone-forming cells. A larger pore size also increases the risk of bacterial contamination. On the other hand, if the pore size is too small, the migration of all cells will be limited.
After GBR, the augmented bone will have a greater volume than before, but gum tissue will remain unchanged. It may be necessary to release the underneath of the gum tissue so it becomes more flexible and can be carefully stretched and stitched over the new bone, without creating too much pressure and tension.
Generally, GBR is a predictable and successful procedure that will regenerate bone within three months or more. It is vital to ensure the deficit does not come under pressure during regeneration. Too much pressure could cause the membrane to collapse, affecting the contour of the newly regenerated area. Patient compliance is also important, as patients must look after the wound during healing and should closely follow all instructions for oral care.
Ridge augmentation
Restorations supported by means of dental implants are currently a highly predictable treatment modality for the rehabilitation of partial and complete edentulism. Advantages of oral implant treatment over conventional non-surgical prosthetic rehabilitation has added to its wide acceptance.
Alveolar ridge, as a part of the periodontium, plays an integral role in the maintenance of both the natural dentition and dental implants. An adequate volume of bone at the siteof implant placement is a necessity to ensure favourable biomechanics and long term esthetic outcome.As reviewed from clinical situations, the minimum dimensions in the maxilla to insert a dental implant are an alveolar ridge width of 5 mm and a bone height of 10 mm. Localized or generalized bone defects of the alveolar ridge can ensue, due to atrophy, prolonged edentulism, congenital anomalies, periodontal disease, infection and post-traumatic causes. These causes in turn may make it impossible to meet the minimum dimensions for implants to be placed. To regain lost bone tissue in height and width, ridge augmentation is employed. Surgical techniques for augmentation involve bone grafting options & non-bone grafting options with ever evolving alternatives. From the systematic reviews, the general consensus is that horizontal ridge augmentation is highly predictable, with good resultant implant survival rates when compared to vertical ridge augmentation.
The advent of osseointegration and advances in biomaterials and techniques have contributed to increased application of dental implants in the restoration of partial and completely edentulous patients. Often, in these patients, soft and hard tissue defects result from a variety of causes, such as infection, trauma, and tooth loss. These create an anatomically less favorable foundation for ideal implant placement. For prosthetic-driven dental implant therapy, reconstruction of the alveolar bone through a variety of regenerative surgical procedures has become predictable; it may be necessary prior to implant placement or simultaneously at the time of implant surgery to provide a restoration with a good long-term prognosis. Regenerative procedures are used for socket preservation, sinus augmentation, and horizontal and vertical ridge augmentation.
Many different techniques exist for effective bone augmentation. The approach is largely dependent on the extent of the defect and specific procedures to be performed for the implant reconstruction. It is most appropriate to use an evidenced-based approach when a treatment plan is being developed for bone augmentation cases.

Root (Part of tooth which is not visible in oral cavity) coverage procedures
The root is the part embedded in the jaw. It anchors the tooth in its bony socket and is normally not visible. The root is attached to the jawbone by a group of specialized connective tissue fibers called the periodontal ligament. A tooth may have one or more roots. Normally, front teeth (incisors, canines) have a single root while molars can have two, three or more roots but this varies from individual to individual.
The periodontal ligament is a specialized connective tissue that attaches the cementum of a tooth to the alveolar bone. They are a network of elastic fibres that help support the tooth inside the alveolar bone socket. The functions of the periodontal ligaments include attachment of the tooth to the bone, support for the tooth, formation, and resorption of bone during tooth movement, sensation, and eruption. When pressure is exerted on a tooth, such as during chewing or biting, the tooth moves slightly in its socket and puts tension on the periodontal ligaments. This is called tooth physiologic mobility. The periodontium exists for the purpose of supporting teeth during their function; a constant state of balance always exists between the periodontal structures and the external forces.
Most of the times, periodontal diseases are caused by bacteria from the dental plaque which is adherent to tooth surfaces. In case of bacterial infections, the first barrier is the gum. In the absence of treatment, the infection progresses to the periodontal ligaments and the alveolar bone involving the progressive loss of the alveolar bone around the teeth which can lead to the loosening and subsequent loss of teeth.